
Spine fixation surgery stabilises a compromised spinal column using advanced implants like rods, plates, and screws to facilitate permanent bone fusion.
For patients experiencing chronic, debilitating back pain or structural instability, knowing exactly when to transition from conservative therapies to advanced surgical evaluation is critical.
In such cases, timely evaluation by an experienced spine fixation surgeon, such as Dr Rohit Mishra in Kolkata, can help identify structural problems early, protect neurological function, and restore long-term spinal stability and mobility.
Quick View: When to Seek a Spine Evaluation
- The Core Indicator: Spine fixation is required when structural instability threatens spinal cord integrity or causes unmanageable mechanical pain.
- Red Flag Symptoms: Immediate consultation is mandatory if you experience progressive neurological deficits, sudden bowel/bladder incontinence, or severe trauma.
- The Specialist: A qualified spine fixation surgeon, such as Dr Rohit Mishra in Kolkata, can accurately diagnose structural spinal issues and determine if stabilisation hardware is required.
- The Goal: Surgical intervention aims to restore structural alignment, decompress neural elements, and eliminate painful segment motion.
Understanding Spinal Instability and Hardware Fixation
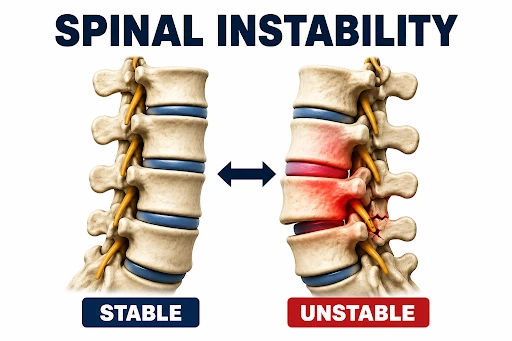
The human spine relies on a delicate balance of bones, discs, and ligaments to protect the spinal cord while allowing fluid movement. When degenerative diseases, severe injuries, or structural defects compromise this stability, the resulting friction and nerve compression cause intense pain.
| Stage | Clinical Progression |
| Initial Structural Problem | Spinal Instability / Severe Disc Collapse |
| Resulting Effect | Mechanical Friction & Nerve Compression |
| Indicators for Surgical Evaluation | Conservative Treatments Fail (Over 6–12 Weeks)Progressive Neurological Deficits SurfaceStructural Alignment Compromised |
| Specialist Intervention | Surgical Intervention by a SpecialistHigh-Precision Decompression of Neural ElementsRigid Hardware Fixation (Pedicle Screws & Rods)Structural Graft Placement for Permanent Fusion |
| Outcome | Spinal Column Stabilised & Neural Pathway Protected |
Spine fixation surgery permanently joins two or more vertebrae. A specialised spine fixation surgeon uses medical-grade titanium screws, rods, or interbody cages to anchor the unstable segments.
This rigid framework acts as an internal splint, holding the bones perfectly still while a bone graft grows together to form a single, solid bone unit.
Emergency Spinal Symptoms: When to Seek Immediate Care
Certain acute spinal symptoms indicate severe neurological compromise. If you experience any of the following red-flag symptoms, bypass standard outpatient wait times and seek emergency surgical evaluation immediately.
Go to the nearest emergency department immediately for an urgent evaluation by a spine fixation surgeon. Dr Rohit Mishra, in Kolkata, offers personalised consultations to prevent permanent neurological paralysis.
Cauda Equina Syndrome
This represents a critical medical emergency caused by massive compression of the lumbosacral nerve roots. It is characterised by saddle anaesthesia (sudden numbness in the groin, buttocks, and inner thighs), accompanied by a sudden loss of bowel or bladder control.
Immediate surgical intervention within 24 to 48 hours is mandatory to prevent permanent lower-body paralysis.
Rapidly Progressive Motor Weakness
Sudden motor deficits, such as foot drop (the inability to lift the front part of your foot while walking), indicate acute nerve root compression.
If you find yourself dragging your toes or suddenly unable to push off your heel, the motor nerves require urgent surgical decompression.
Loss of Balance and Coordination
Difficulty walking in a straight line, unsteadiness on your feet, or a feeling that your legs are heavy and uncoordinated can signal cervical or thoracic myelopathy (spinal cord compression). This requires rapid stabilisation to halt progressive damage.
Chronic Symptoms Requiring Surgical Evaluation
For most individuals, spinal structural failure develops gradually over months or years.
If you experience the following persistent, progressive symptoms for more than 6 to 12 weeks, schedule a comprehensive assessment with a spine fixation surgeon without delay.
1. Severe Mechanical Back Pain
Unlike standard muscle strains that improve with rest, mechanical back pain is directly linked to the physical movement of unstable spinal segments. This condition is clinically marked by:
- Movement-Induced Spikes: Sharp, localised pain that intensifies dramatically during specific movements, such as bending forward, twisting the torso, or transitioning from a sitting to a standing position.
- Inability to Find Relief: A deep, structural aching that does not subside when lying flat, resting, or using standard heat and cold therapies.
- Audible or Physical Sensations: A distinct popping, clicking, or “catching” sensation within the spinal column during movement, indicating abnormal micro-motion between loose or degenerated vertebrae.
2. Persistent Radiculopathy (Sciatica and Nerve Root Pain)
When structural instability causes vertebrae to shift out of alignment, the exit pathways for spinal nerves (the neural foramina) become severely narrowed. This condition is clinically marked by:
- Radiating Electric Shocks: Sharp, burning, or electric shock-like pain that shoots from the lower back down through the buttocks, thighs, and calves (commonly known as sciatica), or from the neck down into the arms and fingers.
- Chronic Numbness and Tingling: A persistent “pins and needles” sensation or total loss of feeling along specific dermatomal nerve pathways in the legs or arms.
- Resistance to Standard Care: Radicular pain that persists for more than six to twelve weeks despite dedicated courses of anti-inflammatory medications and targeted physical therapy.
3. Neurogenic Claudication
Neurogenic claudication is a classic hallmark of advanced central spinal stenosis, often directly associated with the mechanical instability of the lumbar spine. This condition is clinically marked by:
- The Walking Threshold: A predictable onset of cramping, heavy pain, or severe numbness in both legs after walking a short, specific distance.
- The “Shopping Cart” Sign: Leg discomfort that resolves almost immediately when you lean forward at the waist. Leaning forward temporarily widens the spinal canal, relieving pressure on the compressed nerve roots.
4. Progressive Spinal Deformity
Structural conditions like adult-onset scoliosis or severe kyphosis cause the spinal column to curve abnormally. This structural breakdown is clinically marked by:
- Visible Postural Changes: An abnormal forward curvature (hyperkyphosis, often called a “hump”) or a noticeable sideways deviation of the spine (degenerative scoliosis).
- Postural Collapse: Feeling an intense muscular fatigue or a structural “giving way” in the back after standing upright for only a few minutes.
- Significant Loss of Height: A gradual loss of physical height accompanied by mid-to-low back pain, which frequently points to multiple osteoporotic or traumatic vertebral compression fractures
Common Underlying Pathologies Requiring Spinal Fixation

Spinal hardware is not a primary treatment for standard backache; it is explicitly indicated for verified structural pathologies.
During a diagnostic evaluation, Dr Rohit Mishra, an experienced spine fixation surgeon in Kolkata, reviews clinical presentations alongside advanced medical imaging to identify the precise structural pathology.
Spondylolisthesis
This condition occurs when one vertebra slips forward over the bone beneath it. When advanced slippage (Grade II or higher) causes severe mechanical instability, a spine fixation surgeon must realign the slipped bone and secure it in place to prevent further nerve damage.
Traumatic Spinal Fractures
High-impact accidents, falls, or severe osteoporotic collapses can break vertebral bodies. If a fracture compromises the structural stability of the spinal column, immediate fixation surgery is required to protect the spinal cord from permanent injury.
Advanced Degenerative Disc Disease
Severe disc disease causes multiple spinal discs to lose their height entirely, causing raw bone surfaces to rub directly against one another. This bone-on-bone friction creates severe localised inflammation and mechanical instability.
Spinal Tumours and Infections
Primary or metastatic spinal tumours, as well as infections like spinal tuberculosis (Pott’s disease), can aggressively destroy the vertebral bone structure. Hardware fixation is required in these cases to rebuild and stabilise the spinal column after the diseased tissue is removed.
The Threshold for Surgical Intervention
Surgery is considered only when specific clinical thresholds are crossed.
Conservative Management Failure
When targeted physical therapy, core stabilisation exercises, pain medications, and targeted epidural steroid injections fail to provide measurable relief over a 90-day period, the underlying issue is likely mechanical instability that non-surgical therapies can no longer compensate for.
Refractory Pain Control
If your daily pain cannot be managed by maximum safe doses of anti-inflammatory medications or specialised nerve blocks, leaving you homebound or bedridden, the mechanical source of the pain must be structurally corrected.
Severe Impact on Quality of Life
When spinal pain prevents you from performing basic daily tasks, attending work, sleeping consecutively, or walking short distances, the structural benefits of a spinal fusion outweigh the conservative alternatives.
What to Expect During Your Surgical Consultation

A comprehensive initial evaluation with an expert spine fixation surgeon ensures an accurate diagnosis and a highly customised surgical strategy.
Neurological Examination
Your surgeon will carefully evaluate your reflexes, muscle strength across different muscle groups, sensory responses to touch, and your natural walking gait to pinpoint the exact location of nerve compression.
Advanced Diagnostic Imaging Assessment
To map your spinal anatomy precisely, a spine fixation surgeon evaluates three distinct imaging modalities:
- Dynamic X-Rays: These flexion and extension X-rays are taken while you bend forward and backwards to catch abnormal, excessive movement between your vertebrae in real time.
- MRI Evaluation: High-resolution magnetic resonance imaging is used to view the soft tissues. This allows the surgeon to assess disc herniations, spinal cord compression, and nerve root pinching.
- CT Scan Assessment: Computed tomography provides a detailed, three-dimensional view of the bony architecture, which is essential for planning the precise placement of titanium screws and rods.
Take the Next Step Toward Spinal Health
If your symptoms are progressive and conservative treatments are no longer providing relief, speak to Dr Rohit Mishra, the leading spine fixation surgeon in Kolkata.
Call 91473 80550 and book a personalised consultation today.
People Also Ask (PAA)
How does a spine fixation surgeon determine whether surgery is necessary?
A surgeon evaluates spinal stability, nerve involvement, imaging findings, symptom severity, and response to conservative treatments before recommending surgery.
What tests may be required before spinal fixation surgery?
Common tests include blood investigations, ECG, MRI, CT scans, bone density assessment, chest imaging, and dynamic spinal X-rays.
Can spinal instability worsen if left untreated?
Yes. Untreated spinal instability may cause increasing pain, deformity progression, mobility limitations, and worsening nerve compression over time.
Are minimally invasive spine fixation procedures available?
Yes. Minimally invasive techniques use smaller incisions and specialised instruments, depending on spinal anatomy, instability, and diagnosis.
How long does recovery take after spinal fixation surgery?
Recovery varies by procedure complexity and health status. Most patients resume activities gradually within weeks after surgery.
Will spinal fixation limit movement permanently?
Movement decreases at the treated segment, but many patients experience improved mobility due to reduced pain and instability.
What are the possible risks of spinal fixation surgery?
Risks include infection, bleeding, nerve injury, blood clots, hardware complications, delayed fusion, and adjacent segment degeneration.
Can elderly patients undergo spinal fixation surgery safely?
Many elderly patients undergo surgery successfully when overall health, bone quality, and expected benefits support treatment.
How successful is spinal fixation surgery for nerve compression symptoms?
Appropriately selected patients often experience significant relief from pain, numbness, tingling, weakness, and nerve compression symptoms.
What questions should patients ask during a consultation?
Ask about diagnosis, treatment options, expected outcomes, recovery timeline, risks, rehabilitation needs, and activity restrictions.